
Novembro de 2021 – Vol. 26 – Nº 11
Monique Leite Sampaio1,
Nádia Nara Rolim Lima2,
Modesto Leite Rolim Neto3.
1 Obstetrician Gynecologist, Preceptor of the Federal University of Campina Grande – UFCA, Campus Cajazeiras-PB / HUJB
2 Postgraduate Program in Neuro-Psychiatry, Federal University of Pernambuco – UFPE, Recife, Pernambuco, Brazil
3School of Medicine, Federal University of Cariri – UFCA, Barbalha, Brazil.
ABSTRACT:
INTRODUCTION: Maternal death by suicide raises serious perplexities. The ICD-10 classifies maternal suicide as an indirect form of maternal death. Due to this current misclassification, a classificatory consensus of maternal suicide as a direct form of maternal death is urgent.
OBJECTIVE: Analyze the psychological that permeate the phenomenon of maternal suicide, to define the profile of mothers in the postpartum period and pregnant women who commit suicide, with the purpose of elucidating ways of preventing maternal suicide.
METHOD: A systematic review was made following the PRISMA protocol (Preferred Reporting Items for Systematic Reviews and Meta-Analysis).
RESULTS: Twenty-one studies reported the urgent need to implement interventions to prevent or reduce mental health problems caused by mothers and pregnant women who commit suicide. Twenty studies demonstrate the need for interventions to organizational adjustments, especially related to the emotional conflicts involved suicide and maternity.
CONCLUSION: Maternal suicide is caused by severe psychiatric disorders, however, higher suicide rates are seen due to psychosocial factors, such as poor familial support and domestic violence, illegal substance abuse and alcoholism, history of sexual or physical violence, racial oppression, economic instability, unwanted pregnancy, difficulty in accessing intentional abortion, and trauma related to past maternity experiences.
Key words: Maternal death; Suicide; Mental disorders; Pregnancy; Postpartum period
INTRODUCTION
The death of a mother, in of itself, leaves unbearable trauma and irreparable damage not only for the children but for the entire family and social context surrounding the mother. Hence, the struggle for the survival of pregnant women and mothers in the postpartum period has raised great scientific and social efforts, resulting in the global decline of annual rates of maternal death by 46% between the years of 1990 and 2010[1]. Most causes of maternal death, such as hemorrhage, eclampsia, malnutrition, infection, and venous thromboembolism have been combated and mitigated[2,3]. However, little focus has been placed on maternal suicide, which is now characterized as the primary cause of maternal death in developed countries as well as among the leading causes in developing countries[4].
Maternal death is defined by the tenth edition of the International Classification of Diseases (ICD-10) as the death by any means of a pregnant woman up to one year after the end of her pregnancy, whether directly, i.e., pregnancy-related obstetric causes, childbirth, and puerperium, or indirectly, due to non-obstetric or pre-existing conditions, aggravated by the effects of pregnancy [5]. In this context, maternal death by suicide raises serious perplexities. The ICD-10 classifies maternal suicide as an indirect form of maternal death, making these cases even more difficult to classify, analyze, and prevent[6]. Due to this current misclassification, a classificatory consensus of maternal suicide as a direct form of maternal death is urgent[7]. Because of this, the discussion for the eleventh edition of the International Classification of Diseases (ICD-11) has proposed to include suicide as a direct form of maternal death to facilitate its epidemiological analysis, screening, and prevention [4,6,7]. Nevertheless, even with ICD-10 applied the notification and computation of maternal suicides are extremely impaired because there is still no definitive, standard classification; many countries, especially the least developed, still do not classify maternal suicides as direct maternal deaths, leading to an important gap in the knowledge of maternal deaths due to suicide worldwide[4].
During this situation, maternal suicide continues to reach terrifying rates. There are 2 suicides per 100,000 live births in the USA[8] and Canada[9] , while there are 3.7 suicides for every 100,000 in Sweden[10], and 2.3 per 100,000 in Italy[11], with similar rates worldwide. This paper aims to understand the phenomenon of maternal suicide by qualitatively analyzing the relationship between suicide and maternity, characterizing causes, issues, and cofactors involved in the process of maternal suicide, as well as proposing preventative measures. This paper aims to identify who are the mothers and pregnant women who commit suicide.
METHOD
A systematic revision was made, following the PRISMA protocol (Preferred Reporting Items for Systematic Reviews and Meta-Analysis).
Inclusion criteria
To search for studies, the following databases were used: PubMed Scopus and Embase. We identified categorized references for the “Maternal death;” “Suicide;” “Mental disorders;” “Pregnancy;” “Postpartum period.” Besides, we identified references by searching (title/abstract) in the database, using the keywords: suicide *, psych *, stress *, ans *, depr *, mental *. We selected all references identified specifically for the inclusion criteria for this systematic review.
Data extraction and methodological quality assessment
We have developed a data extraction form to collect data on participants and exposure intervention, if relevant, results related to relationship between suicide and maternity, characterizing causes, issues, and cofactors involved in the process of maternal suicide. We extracted data on mental health problems, as well as related ones (that is, risk/resilience factors); strategies implemented or accessed by with the objective to identify who are the mothers and pregnant women who commit suicide.
Three researcher (MLRN, SNAO and NNRL) extracted data and another verified the extraction. Three researchers (KRDA, FC and MMMB) independently assessed the methodological quality of systematic reviews using the AMSTAR tool[46] and qualitative studies using the CASP checklist (Critical Appraisal Skills Program – CASP)[47]. A researcher (MLRN) assessed the quality of cross-sectional studies using the JBI Prevalence or the JBI Cross-sectional analytical checklist and longitudinal studies using the JBI Cohort checklist (Johanna Briggs Institute )[48].
Data presentation and analysis
We summarized the results narratively. We described interventions and outcomes based on the information provided in the studies. We decided not to perform a quantitative analysis of summaries of the associations between the various correlates and health factors, due to a combination of heterogeneity in the measures and lack of control groups, and an embraced lack of descriptions necessary to confirm sufficient homogeneity. We rated the certainty of the evidence using the GRADE approach – (Grading of Recommendations Assessment, Development and Evaluations [49].
RESULTS
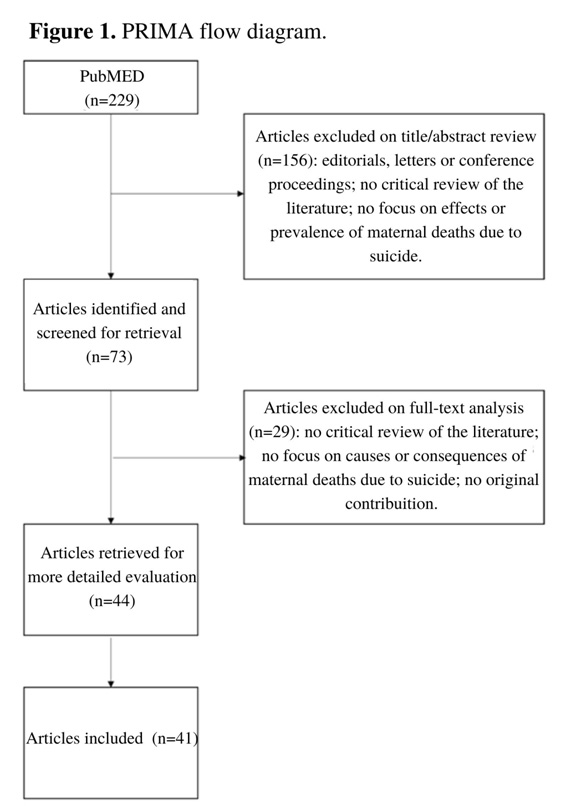
The search strategy yielded 229 results in PubMed Scopus and Embase. Titles and/or abstracts of these records were screened and 156 did not meet the eligibility criteria. Out of the remaining seventy-three full-text articles, thirty-two excluded for assorted reasons, such as lack of relevancy to the proposed topic. Thus, our systematic review includes forty-one publications. (Figure 1 ).
Evaluation of the methodological quality of the included studies
The most common methodological weaknesses in all the studies arose from insufficient reporting: samples, scenarios, and recruitment procedures were often not fully described.
Interventions in mental health
Twenty-one studies reported the urgent need to implement interventions to prevent or reduce mental health problems caused by mothers and pregnant women who commit suicide. Twenty studies demonstrate the need for interventions to organizational adjustments, especially related to the emotional conflicts involved suicide and maternity.
Changes in mental health
Fifteen of the studies that implemented mental health interventions reported the effects of interventions on emotional conflicts involved suicide and maternity. The only data available to connect the impact of the suicide came from three longitudinal research studies, that report changes over time, both of low-quality methodological value.
The summary of the results table below shows the studies that contribute to each mental health result. We evaluate that the certainty of the reported results of levels of anxiety, depression, distress, and sleep problems in pregnant women who commit suicide, using the GRADE approach, is moderate. 3.9.
DISCUSSION
Studies report that motherhood can work as a protective factor for mental health, reducing the risk of suicide, especially in pregnant women and women who have recently given birth [12,13]. However, maternal suicide is a major cause of maternal death around the world, primarily in developed countries [4,14]. Pregnancy and the arrival of a child represent, for many women, a unique experience of hope and joy, but for some women, this period may become overlapped by serious psychiatric disorders, which destabilize and lead to life-threatening situations for many mothers and pregnant women [14, 15]. In this context, motherhood intensifies the prevalence of mental illnesses in vulnerable women [3], with a history of suicidal thoughts, i.e., a set of suicidal behaviors that include intentional self-harm (with or without the intention to die), suicide ideation and suicide attempts [16]. Major depressive disorders during pregnancy and the postpartum period, which is considered a main risk factor for maternal suicide, is heavily prevalent, affecting around 20% of women worldwide, from mild forms to more severe ones and, more rarely, psychosis [4,17]. Inde ed, perinatal depression is a unique subtype of major depressive disorder, where women rapidly experience severe forms of depressive episodes with elevated levels of comorbidities such as anxiety, obsessive-compulsive disorders, and ideations of inflicting self-harm and harm to the child [14,18].
Women in mental distress are more likely to commit suicide [14], in the first months postpartum [13,19] and during the pregnancy [8,19]. Studies confirm this notion, stating that most pregnant women and mothers who commit suicide are afflicted with severe mental illnesses [3], such as major depressive disorders and schizophrenia (Bachmann. 2018; Austin et al., 2007), and account for 75% of all maternal suicides [2,10,20]. Furthermore, high rates of suicidal behavior are also seen in women with a history of illegal substance abuse [19,20,21], alcoholism [19,22, 23], and even tobacco consumption [3]. A study performed in Sri Lanka links the high prevalence of depression in pregnant women, with 27.1% of the pregnant women having a depressive episode prior to the pregnancy and 16.2% having postpartum depression, with the high rate of maternal suicides, which represents 18% of all the causes of maternal deaths in the country [24]. Suicide is also one of the main causes of maternal deaths in other developing countries, but nonetheless, maternal suicide has remained under-investigated and under-diagnosed and consequently under-treated [25]. The social stigma surrounding taking one’s life, as well as inadequate health systems and classificatory obstacles still prevail, which all contribute to the fundamental problem of underreporting [4,25].
In any case, maternal suicide, as with any other psychological phenomenon, does not have one single cause. Pregnant women and mothers in postpartum in such a diverse world could not have the same sufferings nor could they suffer equally in any of their afflictions. However, family support has been shown to be a significant protective factor against maternal suicide [25,26], while mothers without adequate family support have higher rates of suicide [3,25]. Guasia et al. [27] claim that in Bangladesh, unhelpful and unsupportive husbands and mother-in-laws were significant risk factors for suicide, especially for women who have suicidal ideation during pregnancy, which makes up 14% of all pregnant women in the country. In addition, unmarried or divorced marital statuses, as well as pregnancies outside of marriage are also presented as risk factors for maternal suicide, as these situations could be associated with a lack of familial ties and support [21, 28]. On the other hand, marital satisfaction was revealed as a protective factor, due to the emotional support provided [29]. Not surprisingly, teenage mothers may be three times more likely to commit suicide than other age group of women [3, 13.
Likewise, domestic violence has been demonstrated to aggravate the risk of maternal suicide [23,30,31]. In the USA, 54.3% of women who have committed maternal suicide have experienced some type of domestic abuse [8]. In India, Supraja et al. [32] also indicates that domestic violence and inadequate familial and social support has a strong strong correlation with suicidal ideation in early pregnancy. Furthermore, other types of abuse, whether physical or psychological, are also identified as determining factors for maternal suicide [16,21], such as sexual violence, where studies indicate that mothers who were victims of sexual abuse in the antenatal period have 2 to 4 times more symptoms of depression [3].
Social contexts of oppression, such as being an ethnic minority, also proves to be of high significance when examining the suicide of mothers and pregnant women worldwide [25]. In Canada, where 1 in 5 maternal deaths occurs due to suicide or drug toxicity [9], self-harm ideation rates are alarmingly higher in Aboriginal women, who experience different forms of social disparities, than in other groups of Canadian women [33]. Similarly, in the USA, Native American women have been reported to have higher rates of maternal suicide than any other ethnic group [8]. In Sweden, women who have emigrated from developing countries had three times more psychiatric morbidities during postpartum than Swedish immigrants from more developed countries [10]. This situational framework is further intensified in women refugees and asylum seekers, where Collins et al. [34] report that such groups reach three times higher prevalence of post-natal depression due to serious stressful and traumatic life events in the past.
A range of various social settings has been demonstrated to have significant impacts on maternal mental health and, therefore, a direct effect on maternal suicide. Furthermore, unemployment and low wages are already well understood to be related to suicide in the general population [12,25]. Supraja et al. [32] also reports that, in India, the highest prevalence of maternal suicide occurs in middle-class women, potentially due to the unstable and still growing Indian economy, where even the middle class finds themselves lacking financial stability. There is also evidence that lower levels of education, which may be related to low income and unemployment, is a risk factor for suicide, particularly in the first postpartum year [17, 30,35].
Unplanned or unwanted pregnancies are also described as a risk factor for maternal suicide [3,16,]. Thus, difficult access to abortion services, as well as the illegality of abortion in certain countries, also tends to corroborate maternal suffering and suicide [21]. A study conducted in Brazil by Alves et al. [36] associated unwanted pregnancy, the illegality of intentional abortion, and less privileged social condition with maternal suicide, where suicide could present itself as the only resource in the face of the despair of women without adequate familial support. Intentional abortion is also associated with higher rates of maternal suicide in some studies [11,13]. However, the evidence establishes a higher suicide rate after intentional abortion because it stems from traumas experienced during the procedure, and not from the abortion decision or from the act itself [[37]. Miscarriage and the loss of a child in the first year of life are described as extraordinarily strong risk factors for suicidal behavior [29, 38], as well as the sorrow of having a stillborn child [17].
It is important to highlight that the general population of women is less likely to commit violent suicide [10], however, in the case of maternal suicides, most women end up committing suicide violently [39], by hanging or jumping [40]. Thornton et al. [41] refers that, in Australia, 73% of maternal suicide cases were conducted by violent means, some cases including gunshot and lying-in front of a moving object. Maternal distress and suicidal ideation during pregnancy are even associated with gestational and childbirth complications, as well as impairments in the newborn child’s physiology, such as reduced dopamine levels and increased cortisol levels [21].
Revealing the singularity of the phenomenon of maternal suicide, the violent way in which pregnant or in-postpartum women seek to take their own lives opens the complexity of the theme and the severity of the despair suffered by those who do so. Countless reasons can lead women, both in the pregnancy period and in the postpartum period, to attempt violence against their own lives. Many studies are in consensus that maternal suicide presents itself as a serious and unique psychiatric phenomenon despite the social factors strongly associated with suicidal behavior mentioned above [11,14,16,18]. Thus, a history of mental illness such as depression, anxiety, bipolarity, post-traumatic stress disorder, suicide ideation, substance abuse, or any other effect of psychotic disorder, in addition to a family history of psychiatric diseases and suicide is a primary risk factor for maternal suicide [12,14,15,21,28,32].
The death of a pregnant or a puerperal woman by suicide is a tragedy of incalculable damage, which carries immeasurable psychological damage for the entirety of their life [42]. The descendants of mothers who come to commit suicide are at an increased risk of also committing suicide [43], in addition to being prone to numerous other psycho-emotional disorders [42,44,45]. Lieb et al. [45] still indicate that suicidal behavior may have genetic factors involved as well, as though suicide could run in families. Therefore, antenatal treatment of depression can prevent higher rates of suicide in the offspring [35].
CONCLUSION
Women who commit maternal suicide are, above all, women with serious mental illnesses[14,15,18], and with suicide aggravated by serious situations of psychosocial vulnerabilities, those of which include poor familial support[26,29], domestic abuse [30,31], a history of sexual abuse[3], illegal substance abuse and alcoholism[20,22,23], specific racial oppression[10,33], economic instability[17,32], and unwanted pregnancy combined with difficulty or illegality to perform intentional abortion[36], in addition to severe trauma related to motherhood, such as miscarriage and loss of child during the delivery or within the first year of life[38] .
Considering that pre-existing mental illness is strongly associated with most suicide cases, maternal suicides must be considered preventable with adequate medical care, especially with primary health care [6]. With the universal and systematic screening of mental illness in the earlier stages of pregnancy [19,44], about a quarter of all maternal suicides could be prevented [40], with adequate pharmacological therapy and comprehensive psychological assistance [38]. Regarding the profile of pregnant women and mothers in the postpartum period who have committed suicide, it is imperative to develop multidisciplinary monitoring standards for the preventative care for suicide in women defined as most vulnerable [2,44] in all levels of care [25]. Special treatments must be focused mainly on pregnant women who have related a past of psychiatric disorders or addictions[19,23], or even a history of suicide in the family[12], with great attention given to unmarried women, unemployed women, women in the course of unwanted pregnancy, those who have suffered from traumatic experiences, such as physical or sexual violence, those who lack adequate support from family and those belonging to marginalized social groups[20,21,34]. Furthermore, there is an urgent need for a consensus on the classification of maternal suicide [4], to avoid misclassification bias and enable better analysis of the theme [6,7,15].
REFERENCES
- WHO, World Health Organization, World Bank, United Nations Population Fund & United Nations Children’s Fund (UNICEF)? (2012). Trends in maternal mortality: 1990 to 2010: WHO, UNICEF, UNFPA and The World Bank estimates. https://apps.who.int/iris/handle/10665/44874
- Metz, T. D., Rovner, P., Hoffman, M. C., Allshouse, A. A., Beckwith, K. M., & Binswanger, I. A. (2016). Maternal Deaths from Suicide and Overdose in Colorado, 2004-2012. Obstetrics and gynecology, 128(6), 1233–1240. https://doi.org/10.1097/AOG.0000000000001695
- Gavin, A. R., Lindhorst, T., & Lohr, M. J. (2011). The prevalence and correlates of depressive symptoms among adolescent mothers: results from a 17-year longitudinal study. Women & health, 51(6), 525–545. https://doi.org/10.1080/03630242.2011.606355
- Fuhr, D. C., Calvert, C., Ronsmans, C., Chandra, P. S., Sikander, S., De Silva, M. J., & Patel, V. (2014). Contribution of suicide and injuries to pregnancy-related mortality in low-income and middle-income countries: a systematic review and meta-analysis. The lancet. Psychiatry, 1(3), 213–225. https://doi.org/10.1016/S2215-0366(14)70282-2
- WHO? World Health Organization. (2019) International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). Version for 2019. Available in: https://icd.who.int/browse10/2019/en
- Hasegawa, J, Katsuragi, S, Tanaka, H, Kubo, T, Sekizawa, A, Ishiwata, I, Ikeda, T. (2020). How should maternal death due to suicide be classified? Discrepancy between ICD‐10 and ICD-MM. BJOG; 127: 665– 667. https://doi.org/10.1111/1471-0528.16087
- Lommerse, K., Knight, M., Nair, M., Deneux-Tharaux, C., & van den Akker, T. (2019). The impact of reclassifying suicides in pregnancy and in the postnatal period on maternal mortality ratios. BJOG: an international journal of obstetrics and gynaecology, 126(9), 1088–1092. https://doi.org/10.1111/1471-0528.15215
- Palladino, C. L., Singh, V., Campbell, J., Flynn, H., & Gold, K. J. (2011). Homicide and suicide during the perinatal period: findings from the National Violent Death Reporting System. Obstetrics and gynecology, 118(5), 1056–1063. https://doi.org/10.1097/AOG.0b013e31823294da
- Jago, C. A., Crawford, S. G., Gill, S. J., & Gagnon, L. (2020). Mental Health and Maternal Mortality-When New Life Doesn’t Bring Joy. Journal of obstetrics and gynecology Canada: JOGC = Journal d’obstetrique et gynecologie du Canada: JOGC, S1701-2163(20)30532-6. Advance online publication. https://doi.org/10.1016/j.jogc.2020.06.016
- Esscher, A., Essén, B., Innala, E., Papadopoulos, F. C., Skalkidou, A., Sundström-Poromaa, I., & Högberg, U. (2016). Suicides during pregnancy and 1 year postpartum in Sweden, 1980-2007. The British journal of psychiatry: the journal of mental science, 208(5), 462–469. https://doi.org/10.1192/bjp.bp.114.161711
- Lega, I., Maraschini, A., D’Aloja, P., Andreozzi, S., Spettoli, D., Giangreco, M., Vichi, M., Loghi, M., Donati, S., & Regional maternal mortality working group (2020). Maternal suicide in Italy. Archives of women’s mental health, 23(2), 199–206. https://doi.org/10.1007/s00737-019-00977-1
- Qin, P., Agerbo, E., & Mortensen, P. B. (2003). Suicide risk in relation to socioeconomic, demographic, psychiatric, and familial factors: a national register-based study of all suicides in Denmark, 1981-1997. The American journal of psychiatry, 160(4), 765–772. https://doi.org/10.1176/appi.ajp.160.4.765
- Mendez-Bustos, P., Lopez-Castroman, J., Baca-García, E., & Ceverino, A. (2013). Life cycle and suicidal behavior among women. TheScientificWorldJournal, 2013, 485851. https://doi.org/10.1155/2013/485851
- Jones, I., Chandra, P. S., Dazzan, P., & Howard, L. M. (2014). Bipolar disorder, affective psychosis, and schizophrenia in pregnancy and the post-partum period. Lancet (London, England), 384(9956), 1789–1799. https://doi.org/10.1016/S0140-6736(14)61278-2
- Austin, M. P., Kildea, S., & Sullivan, E. (2007). Maternal mortality and psychiatric morbidity in the perinatal period: challenges and opportunities for prevention in the Australian setting. The Medical journal of Australia, 186(7), 364–367. PMID: 17407434.
- Castro e Couto, T., Brancaglion, M. Y., Cardoso, M. N., Faria, G. C., Garcia, F. D., Nicolato, R., Aguiar, R. A., Leite, H. V., & Corrêa, H. (2016). Suicidality among pregnant women in Brazil: prevalence and risk factors. Archives of women’s mental health, 19(2), 343–348. https://doi.org/10.1007/s00737-015-0552-x
- Lysell, H., Dahlin, M., Viktorin, A., Ljungberg, E., D’Onofrio, B. M., Dickman, P., & Runeson, B. (2018). Maternal suicide – Register based study of all suicides occurring after delivery in Sweden 1974-2009. PloS one, 13(1), e0190133. https://doi.org/10.1371/journal.pone.0190133
- Galea, L., & Frokjaer, V. G. (2019). Perinatal Depression: Embracing Variability toward Better Treatment and Outcomes. Neuron, 102(1), 13–16. https://doi.org/10.1016/j.neuron.2019.02.023
- Orsolini, L., Valchera, A., Vecchiotti, R., Tomasetti, C., Iasevoli, F., Fornaro, M., De Berardis, D., Perna, G., Pompili, M., & Bellantuono, C. (2016). Suicide during Perinatal Period: Epidemiology, Risk Factors, and Clinical CorreFrontiers in psychiatry, 7, 138. https://doi.org/10.3389/fpsyt.2016.00138
- Bachmann S. (2018). Epidemiology of Suicide and the Psychiatric Perspective. International journal of environmental research and public health, 15(7), 1425. https://doi.org/10.3390/ijerph15071425
- Gentile S. (2011). Suicidal mothers. Journal of injury & violence research, 3(2), 90–97. https://doi.org/10.5249/jivr.v3i2.98
- Singal D, Brownell M, Chateau D, Wall-Wieler E, Longstaffe S, Hanlon-Dearman A, Roos LL (2017). Suicide and suicide attempts among women in the Manitoba Mothers and Fetal Alcohol Spectrum Disorder cohort: a retrospective matched analysis using linked administrative data. CMAJ Open. 17;5(3): E646-E652. doi: 10.9778/cmajo.20160127.
- Crandall, M., Sridharan, L., & Schermer, C. (2010). Depression and thoughts of death among disadvantaged mothers: risk factors and impact on maternal and child health. Archives of suicide research: official journal of the International Academy for Suicide Research, 14(3), 248–260. https://doi.org/10.1080/13811118.2010.494143
- Agampodi, S., Wickramage, K., Agampodi, T., Thennakoon, U., Jayathilaka, N., Karunarathna, D., & Alagiyawanna, S. (2014). Maternal mortality revisited: the application of the new ICD-MM classification system in reference to maternal deaths in Sri Lanka. Reproductive health, 11(1), 17. https://doi.org/10.1186/1742-4755-11-17
- Fisher, J., Cabral de Mello, M., Patel, V., Rahman, A., Tran, T., Holton, S., & Holmes, W. (2012). Prevalence and determinants of common perinatal mental disorders in women in low- and lower-middle-income countries: a systematic review. Bulletin of the World Health Organization, 90(2), 139G–149G. https://doi.org/10.2471/BLT.11.091850
- Chen, Y. H., & Lau, G. (2008). Maternal deaths from suicide in Singapore. Singapore medical journal, 49(9), 694–697. PMID: 18830543.
- Gausia, K., Fisher, C., Ali, M., Oosthuizen, J. (2009). Antenatal depression and suicidal ideation among rural Bangladeshi women: A community-based study. Archives of women’s mental health. 12. 351-8. https://doi.org/10.1007/s00737-009-0080-7.
- Huang, H., Faisal-Cury, A., Chan, Y., Tabb, K., Katon, W., Menezes, P (2012). Suicidal ideation during pregnancy: prevalence and associated factors among low-income women in São Paulo, Brazil. Arch Womens Ment Health15, 135–138. https://doi.org/10.1007/s00737-012-0263-5
- Shi, P., Ren, H., Li, H., & Dai, Q. (2018). Maternal depression and suicide at immediate prenatal and early postpartum periods and psychosocial risk factors. Psychiatry research, 261, 298–306. https://doi.org/10.1016/j.psychres.2017.12.085
- Gelaye, B., Kajeepeta, S., & Williams, M. A. (2016). Suicidal ideation in pregnancy: an epidemiologic review. Archives of women’s mental health, 19(5), 741–751. https://doi.org/10.1007/s00737-016-0646-0
- Alhusen, J. L., Frohman, N., & Purcell, G. (2015). Intimate partner violence and suicidal ideation in pregnant women. Archives of women’s mental health, 18(4), 573–578. https://doi.org/10.1007/s00737-015-0515-2
- Supraja, T. A., Thennarasu, K., Satyanarayana, V. A., Seena, T. K., Desai, G., Jangam, K. V., & Chandra, P. S. (2016). Suicidality in early pregnancy among antepartum mothers in urban India. Archives of women’s mental health, 19(6), 1101–1108. https://doi.org/10.1007/s00737-016-0660-2
- Bowen, A., Stewart, N., Baetz, M., Muhajarine, N. (2009). Antenatal depression in socially high-risk women in Canada. Journal of epidemiology and community health. 63. 414-6. https://doi.org/10.1136/jech.2008.078832.
- Collins, C. H., Zimmerman, C., & Howard, L. M. (2011). Refugee, asylum seeker, immigrant women and postnatal depression: rates and risk facArchives of women’s mental health, 14(1), 3–11. https://doi.org/10.1007/s00737-010-0198-7
- Pearson, R. M., Evans, J., Kounali, D., Lewis, G., Heron, J., Ramchandani, P. G., O’Connor, T. G., & Stein, A. (2013). Maternal depression during pregnancy and the postnatal period: risks and mechanisms for offspring depression at age 18 years. JAMA psychiatry, 70(12), 1312–1319. https://doi.org/10.1001/jamapsychiatry.2013.2163
- Alves, M., Alves, S., Antunes, M., & Santos, D. (2013). Causas externas e mortalidade materna: proposta de classificacao. Revista de Saúde Pública, 47(2), 283-291. https://doi.org/10.1590/S0034-8910.2013047003642
- Reardon, D. C., & Thorp, J. M. (2017). Pregnancy associated death in record linkage studies relative to delivery, termination of pregnancy, and natural losses: A systematic review with a narrative synthesis and meta-analysis. SAGE open medicine, 5, 2050312117740490. https://doi.org/10.1177/2050312117740490
- Tabb, K. M., Gavin, A. R., Guo, Y., Huang, H., Debiec, K., & Katon, W. (2013). Views and experiences of suicidal ideation during pregnancy and the postpartum: findings from interviews with maternal care clinic patients. Women & health, 53(5), 519–535. https://doi.org/10.1080/03630242.2013.804024
- Knasmüller, P., Kotal, A., König, D., Vyssoki, B., Kapusta, N., & Blüml, V. (2019). Maternal suicide during pregnancy and the first postpartum year in Austria: Findings from 2004 to 2017. Psychiatry research, 281, 112530. https://doi.org/10.1016/j.psychres.2019.112530
- Oates M. (2003). Perinatal psychiatric disorders: a leading cause of maternal morbidity and mortality. British medical bulletin, 67, 219–229. https://doi.org/10.1093/bmb/ldg011
- Thornton, C., Schmied, V., Dennis, C. L., Barnett, B., & Dahlen, H. G. (2013). Maternal deaths in NSW (2000-2006) from nonmedical causes (suicide and trauma) in the first year following birth. BioMed research international, 2013, 623743. https://doi.org/10.1155/2013/623743
- Bronisch, T., & Lieb, R. (2008). Maternal suicidality and suicide risk in offspring. The Psychiatric clinics of North America, 31(2), 213–221. https://doi.org/10.1016/j.psc.2008.01.003
- Kuramoto, S. J., Stuart, E. A., Runeson, B., Lichtenstein, P., Långström, N., & Wilcox, H. C. (2010). Maternal or paternal suicide and offspring’s psychiatric and suicide-attempt hospitalization risk. Pediatrics, 126(5), e1026–e1032. https://doi.org/10.1542/peds.2010-0974
- Stein, A., Pearson, R. M., Goodman, S. H., Rapa, E., Rahman, A., McCallum, M., Howard, L. M., & Pariante, C. M. (2014). Effects of perinatal mental disorders on the fetus and child. Lancet (London, England), 384(9956), 1800–1819. https://doi.org/10.1016/S0140-6736(14)61277-0
- Lieb, R., Bronisch, T., Höfler, M., Schreier, A., & Wittchen, H. U. (2005). Maternal suicidality and risk of suicidality in offspring: findings from a community study. The American journal of psychiatry, 162(9), 1665–1671. https://doi.org/10.1176/appi.ajp.162.9.1665.
- Shea, B.J., Reeves, B.C., Wells, G., et al., 2017. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 358, j4008. https://doi.org/10.1136/bmj.j4008. published Online First: 2017/09/25].
- Critical Appraisal Skills Programme (CASP). CASP checklist for qualitative research 2018 [20 March 2020]. Available from: https://casp-uk.net/casp-tools-checklists.
- Johanna Briggs Institute. Critical Appraisal Tools 2018 [Available from: http:// joannabriggs-webdev.org/research/critical-appraisal-tools.html accessed 20 March 2020.
- Guyatt, G., Oxman, A.D., Akl, E.A., et al., 2011. GRADE guidelines: 1. IntroductionGRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 64 (4), 383–394. https://doi.org/10.1016/j.jclinepi.2010.04.026. published Online First: 2011/01/05].
Correspondence:
Modesto Leite Rolim Neto, Faculty of Medicine, Federal University of Cariri (UFCA), 284, Divine Savior Street, Downtown, Barbalha, Ceará 63180000, Brazil
Tel +5588 999042979
Email: [email protected]